Guide to SOAP Notes: How to Write SOAP Notes with Examples & Best Practices

This guide will help you master the art of SOAP note writing, providing you with tools to create proficient and client-centric documentation.
We’ll start with an introduction to the SOAP note format. Then, we’ll discuss insights into what to include in your SOAP notes and how to format them effectively, with examples across multiple disciplines.
Understanding SOAP notes
SOAP notes are a tool for documenting what the client says, what the allied health practitioner observes, the diagnosis or assessment, and the plan for the client’s care.
As common as this note-taking style has become, you might be wondering about the format’s origins and how it stacks up against other note-taking conventions.
Definition & history of SOAP notes
SOAP stands for Subjective, Objective, Assessment, and Plan (in that order). It’s a method of note-taking that allied health professionals use to record and review ongoing client care.
SOAP notes were introduced in the 1960s by Dr. Lawrence Weed, known for his work in medical record standardization. His vision was to improve the quality of client care by creating standard client documentation systems, and the success of his pioneering is evident in the broad use of SOAP notes in allied health today.
The purpose & significance of SOAP notes in client care
SOAP notes are a documentation tool that helps ensure clinical notes are recorded accurately and addressed with an appropriate treatment plan.The SOAP format provides structure and guides practitioners through each of the necessary elements of quality clinical documentation.
SOAP vs other types of clinical notes
While SOAP notes are widely used, they’re not the only option for clinical documentation.
Other types of clinical notes include DAP (Data, Assessment and Plan) and GIRP (Goals, Interventions, Response and Plan), among others. Each type of note has its place in client care.
Like SOAP notes, DAP notes focus largely on the data gathered during the client’s visit.
GIRP notes, on the other hand, focus on the client’s goals, the interventions used by the clinician, the client’s response to these interventions, and the plan moving forward.
Key components of a SOAP note
Let’s explore the components of a SOAP note in detail, along with formatting tips to help ensure your documentation is clear and concise.
Subjective: Capturing the client’s voice
This section covers the client’s perspective. Document the client’s history, symptoms, and concerns exactly as they express them.
Use direct quotes when possible. Begin with the client’s stated reason for the current visit and include relevant client history and symptoms.
Possible subheadings to guide the format of this section are listed below:
- History of Present Illness (HPI): This may include stated symptoms, a chronological history of the client’s medical or mental health complaints, and information obtained from other sources (identify the source if it’s not the client).
- History: This might include medical history, family history, and/or social history.
- Review of symptoms: This involves a set of questions designed to help the client identify symptoms they might previously have overlooked.
- Current medications or allergies: Include this information under the Subjective or Objective sections, if applicable to your practice. Record all current medications and allergies reported by the client. Include the medication name, dose, route, and frequency of intake.
Objective: The facts & figures
This part must include tangible, measurable data. Include vital signs, affect, physical state, test results, and other observable data.
Use clear, precise language. Present data in a logical order, and ensure all measurements and findings are recent, objective, and accurate.
Observations may include:
- Vital signs
- Physical exam findings
- Laboratory data
- Imaging results
- Mood and affect
- Posture
- Other diagnostic data
- Recognition and review of the documentation of other clinicians.
Bear in mind
Symptoms are what the client reports (that’s why they’re under the Subjective section of SOAP notes), whereas the Objective section should cover what you observe.
Assessment: Making sense of the information
Here, you’ll collate your clinical assessments and diagnoses based on information recorded in the Subjective and Objective sections.
Arrange your thoughts clearly. Start with the primary diagnosis, followed by secondary ones (a differential diagnosis) if applicable. Briefly justify your diagnoses with supporting data.
Here’s a formatting example:
- Problem: Here, you’ll list the “problems” (or diagnoses), based on your assessment of the above information. Best practice is to list these in order of importance or urgency.
- Differential Diagnosis: List all possible diagnoses, even the ones that are less probable. Under this subheading, you’ll explain your decision-making process in detail and justify your thought process.
Plan: Mapping out the road ahead
This section outlines the treatment plan, follow-up appointments, and client education. Mention specific medications, therapies, referrals to specialists or recommended lifestyle changes.
Be specific and action-oriented. Include timelines, dosage for medications if applicable, and clear instructions for follow-up.
The following may be helpful for your Plan format:
- Record your recommendations for possible further tests and reasons for recommending each test
- Further interventions needed
- Specialist referral(s)
- Client education
Remember
The key to effective and professional SOAP notes is clarity and brevity. Each section should be concise yet comprehensive, providing all needed information without unnecessary detail.
This approach ensures that your SOAP notes are useful for your practice and other healthcare professionals involved in the client’s care.
SOAP note examples across specialties
Let’s look at hypothetical SOAP note examples from different specialties.
Example 1: SOAP note format example for nurses
Subjective
The patient stated, “I’ve been feeling very tired lately.” The patient reports that “this fatigue is overwhelming” and that onset began approximately 3 months ago, making her “demanding job responsibilities” challenging to fulfill. The patient confirmed that she is not currently taking any medication or supplements. She further noted that, “I struggle to fall asleep and always wake up tired.”
Objective
BP 135/85, HR 78, fatigued appearance and affect.
Assessment
- Diagnosis: Possible dehydration, possible overexertion.
- Differential Diagnosis: Possible deficiencies (such as D3 or B12, known to cause fatigue if severe).
Plan
-
For Immediate Action: Recommend increased fluid intake and electrolytes, as well as improved sleep routine, and prescribe a mild sleep aid. Follow-up appointment scheduled in 7 days.
-
Tests: Bloods were taken to test for the following deficiencies: D3 Iron Magnesium B12
-
D3
-
Iron
-
Magnesium
-
B12
-
Follow-up: Test results due in 5 days, upon which a possible reevaluation of the plan may be needed.
-
D3
-
Iron
-
Magnesium
-
B12
Example 2: SOAP note format example for physical therapists
Subjective
The client reports persistent knee pain worsening over the last month, especially when climbing stairs. The client shared that he was a competitive runner for 15 years but has “been out of action” for 5 years. Client states that he is a “very healthy eater” and continues to “push” himself during physical exercise.
Objective
Swelling observed in the right knee. Limited range of motion to 90 degrees. Pain score upon palpation: 7/10.
Assessment
- Problem: Suspected meniscal injury based on symptom description and physical findings.
- Differential diagnosis: Gout, although this is unlikely based on the patient’s reported lifestyle. Possible referred pain.
Plan
Initiate ultrasound therapy and knee-strengthening exercises. Two appointments per week booked.
Re-evaluate in one week.
Example 3: SOAP note format example for mental health practitioners
Subjective
The client expresses feeling “overwhelmed” after being promoted two months ago, as well as unexplained bouts of “dizziness and a racing heart” while at work. She reported “finding it hard to fall asleep” due to “thinking and worrying about work.”
She confirms that, on average, she sleeps less than 4 hours per night, as she prefers to work late and rise early to “get ahead” of her day. She describes herself as a “perfectionist” and often spends more time than she intended on a task. She likes to be seen as capable and productive and fears disappointing her employer and colleagues.
The client reports that she finds it hard to ask for help and talk about her feelings with others and has only sought counseling after being directed to do so by her employer.
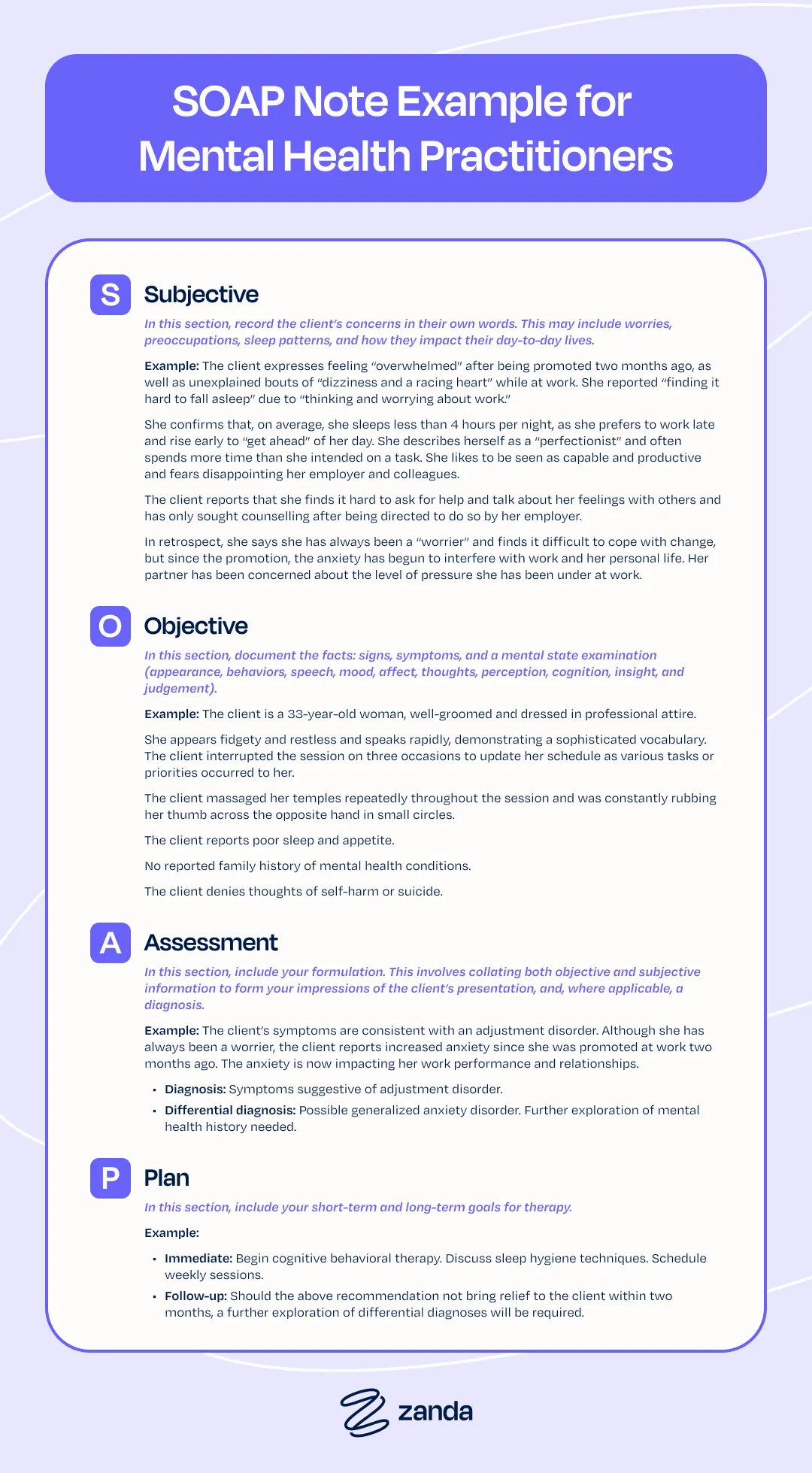
In retrospect, she says she has always been a “worrier” and finds it difficult to cope with change, but since the promotion, the anxiety has begun to interfere with work and her personal life. Her partner has been concerned about the level of pressure she has been under at work.
Objective
The client is a 33-year-old woman, well-groomed and dressed in professional attire.
She appears fidgety and restless and speaks rapidly, demonstrating a sophisticated vocabulary. The client interrupted the session on three occasions to update her schedule as various tasks or priorities occurred to her.
The client massaged her temples repeatedly throughout the session and was constantly rubbing her thumb across the opposite hand in small circles.
The client reports poor sleep and appetite.
No reported family history of mental health conditions.
The client denies thoughts of self-harm or suicide.
Assessment
The client’s symptoms are consistent with an adjustment disorder. Although she has always been a worrier, the client reports increased anxiety since she was promoted at work two months ago. The anxiety is now impacting her work performance and relationships.
- Diagnosis: Symptoms suggestive of adjustment disorder.
- Differential diagnosis: Possible generalized anxiety disorder. Further exploration of mental health history needed.
Plan
- Immediate: Begin cognitive behavioral therapy. Discuss sleep hygiene techniques. Schedule weekly sessions.
- Follow-up: Should the above recommendation not bring relief to the client within two months, a further exploration of differential diagnoses will be required.
Example 4: SOAP note format example for occupational therapy
Subjective
The patient describes difficulty in gripping objects post-wrist fracture recovery.
Objective
Reduced grip strength in the right hand. Struggles with fine motor tasks.
Assessment
Limited hand dexterity and strength, likely due to prolonged immobilization.
Plan
Implement hand exercises focusing on grip strengthening. Introduce adaptive tools for daily tasks. Review in two weeks.
Adapt as you go.
In each of the above examples, the basic SOAP structure is maintained, but the content is tailored to suit the focus of each specialty.
Whether it’s the precise physical measurements in physical therapy, the exploration of thoughts and feelings in mental health, a focus on daily living activities in occupational therapy, or the specific muscle groups in massage therapy, the SOAP format’s flexibility makes it a valuable tool in a wide range of clinical settings.
Formatting recommendations for SOAP notes
Creating SOAP notes that are both informative and efficient requires attention to structure and a balance between detail and conciseness.
Here are some formatting recommendations to help you craft SOAP notes that effectively communicate client information while being easy to read and use.
Structure: Bullet points vs. paragraph form
- Bullet points: Use bullet points for clarity and quick reference. They’re ideal for listing symptoms, observations and action items, making it easier to scan the document.
- Paragraph form: Use this for the Subjective and Assessment sections, where a narrative style is needed to convey the client’s story or a comprehensive assessment.
- Combination approach: Consider combining both forms. For example, use bullet points in the Objective section for clear data presentation and paragraph form in the Subjective section for detailed client history.
Balancing comprehensive and concise documentation
- Relevance is key: Focus on what’s relevant to the client’s current condition and treatment plan.
- Clarity and brevity: Strive for notes that are clear and to the point. Use simple, direct language and avoid industry jargon.
- Consistency: Maintain a consistent level of detail across all sections. This helps create a coherent picture of the client’s condition and care plan.
Remember, the primary goal of SOAP notes is effective communication.
SOAP notes should provide a clear, concise, and comprehensive record that supports client care and facilitates collaboration among healthcare providers.
Benefits of different SOAP note approaches
SOAP notes can be formatted using different styles, each offering unique benefits in specific clinical scenarios. These approaches can be classified as client-centered or problem-centered, both having significant impacts on client outcomes and healthcare team efficiency.
Let’s dive into a comparison of these approaches:
SOAP note formatting styles & their clinical benefits
- Narrative style: This style is beneficial in mental health or counseling settings where understanding the client’s story and perspective is crucial. It allows for a detailed account of the client’s experiences and feelings.
- Bulleted or checklist style: Often used in fast-paced environments like emergency rooms or urgent care, this style allows for quick information retrieval and efficient documentation.
- Hybrid style: Combining narrative and bulleted formats, this approach works well in settings like family medicine or chronic care management, where both detailed descriptions and quick data references are needed.
Client-centered vs. problem-centered approaches
- Client-centered approach: This approach focuses on the client’s overall experience, feelings and perceptions. It’s beneficial in therapeutic settings, promoting a holistic view of the client’s well-being.
- Problem-centered approach: This approach is more focused on specific medical or physical issues. It can be effective in acute care or when dealing with a specific diagnosis.
Impact on client outcomes & healthcare team efficiency
- Client outcomes: Good SOAP note formatting, whether client-centered or problem-centered, ensures that all relevant information is captured and easily accessible. This can lead to more accurate diagnoses, tailored treatment plans and better overall client outcomes.
- Healthcare team efficiency: Efficient SOAP note formatting enables quicker information retrieval and easier communication among healthcare professionals. This can result in better coordination of care, reduced errors and more efficient use of healthcare resources.
The choice of SOAP note formatting and approach should be guided by the specific needs of the clinical setting and the nature of the client’s condition. Both client-centered and problem-centered approaches have their place in healthcare, or even a thoughtful combination of both, tailored to each client’s and situation’s individual needs.
Adapting SOAP notes to modern healthcare challenges
Healthcare is continually evolving. SOAP notes must adapt to changes, particularly in the realms of telehealth and remote monitoring.
Telehealth & remote client monitoring in SOAP notes
- Telehealth services: In telehealth appointments, the Subjective section becomes even more crucial, as healthcare providers may rely more on client-reported symptoms in the absence of traditional physical exams.
- Remote monitoring: Whether offering telehealth or in-person services to clients, the Objective section of your SOAP notes might include data from remote monitoring devices.
Adapting SOAP notes to today’s healthcare challenges not only ensures the notes remain a relevant and powerful tool but also enhances client care in an increasingly digital and interconnected healthcare environment.
Legal & ethical considerations of SOAP notes
Understanding the legal and ethical dimensions of SOAP notes is crucial for any allied health professional.
Legal implications of SOAP notes in client care
SOAP notes can play a role in legal scenarios, such as malpractice lawsuits or insurance claims. They provide a clear, time-stamped record of client care. It’s essential to ensure that notes are accurate, timely, and complete.
A key factor is adherence to regulatory standards. SOAP notes should comply with laws and regulations governing client records. This includes following guidelines for documentation and records retention.
Ethical guidelines for documenting sensitive client information
SOAP notes often contain sensitive data, and the allied health practitioner has a responsibility to protect this information.
This means being vigilant about who has access to notes and how they’re stored and shared.
When documenting sensitive information, it’s important to be respectful and non-judgmental. The language used should be professional and focused on the client’s care and well-being.
Finally, be especially aware of the regulations in your federal or national jurisdiction–it’s the difference between running a thriving and compliant practice and reputational damage.
Zanda security certifications
The security of electronic health records like SOAP notes is essential.
Designed with security measures to protect sensitive client information, Zanda is ISO 27001-certified. Moreover, the software is HIPAA-compliant and GDPR-compliant. It’s also an Australian Cyber Security Centre Partner and is compliant with the Australian Privacy Act. Last but not least, Zanda is POPIA-, CCPA-, and PIPEDA-compliant. The software’s adherence to international privacy laws ensures that data is handled with the utmost care.
Integrating SOAP notes into clinical practice
Now that we’ve covered the fundamentals and best practices for SOAP notes, let’s focus on integrating them into your clinical practice.
Strategies for efficient SOAP note-taking
Here are a few tips for efficient notes:
- Use Standard Templates: Use consistent templates for your SOAP notes, so you’re not starting from scratch at each appointment.
- Regular Training: Engage in regular training sessions. Keeping up to date with best practices can improve the quality and efficiency of your note-taking.
The role of technology in SOAP note documentation
Electronic health records (EHRs) and practice management software like Zanda offer intuitive, secure platforms for creating, storing, and managing clinical notes.
Features like configurable templates, an AI Scribe for clinics, easy access to client information, and secure data storage make technology indispensable in today’s healthcare practices.
Training & resources for healthcare professionals
Ongoing training and access to quality resources are essential for mastering SOAP notes. Zanda provides resources to help healthcare professionals write clinical notes more efficiently.
Depending on your allied health discipline, there are many professional bodies offering further training on clinical note-taking. Incorporating professional development into your practice not only enhances the quality of SOAP notes but also helps ensure your documentation process is as efficient and effective as possible.

Conclusion
As healthcare continues to change, our approaches to documentation should too. Embracing ongoing learning and adaptation in documentation practices is crucial for healthcare professionals striving to provide the best possible care.
Zanda offers a platform to create secure, professional SOAP notes, tailored to the needs of healthcare practices. Our system is designed to make documenting care as seamless and efficient as possible, allowing you to focus more on your clients and less on paperwork.
Experience this ease and efficiency firsthand with a 14-day FREE TRIAL – no credit card required. It’s an opportunity to explore how advanced tools and templates can enhance your documentation practices.